Statistical overview (2004–2020)
The MPDRC (and previously the Obstetrical Care Review Committee) has generated recommendations since being established in 1994. Over time, not only has the committee evolved, but so too have medical technologies, policies, procedures, and public and professional attitudes towards maternal and perinatal care in the province. In order to provide an analysis that is reflective of more current values and attitudes, the statistical analysis contained within this annual report will focus on cases reviewed and recommendations made since 2004.
From 2004–2020, the MPDRC has reviewed a total of 487 cases. Of these cases, 184 (38%) were maternal, 206 (42%) were neonatal and 97 (20%) were stillbirths. These numbers reflect the policy of the OCC to review all maternal deaths. Commencing in 2015, deaths involving women who were pregnant, but where the pregnancy did not cause or contribute to the death, are noted and undergo an “executive” review. The executive review is conducted by a core team of representatives of the MPDRC and includes an analysis of the circumstances surrounding the maternal death. The results of the review are discussed with the full committee for any additional investigation or comment. If necessary and suggested by the broader committee, an executive review may result in a full review. The statistics below reflect the total number of reviews (i.e., executive and full), conducted by the MPDRC.
Neonatal and stillbirth reviews are conducted only when the family, investigating coroner or Regional Supervising Coroner have concerns about the care that the mother or child received.
The number of cases noted in Chart One is based on the year the case was reviewed, which, in many cases, is not the same year in which the death occurred.
| Cases | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | Total | Percent % |
average/year |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total cases reviewed | 30 | 30 | 25 | 27 | 30 | 46 | 41 | 30 | 32 | 26 | 10 | 31 | 26 | 19 | 27 | 34 | 23 | 487 | no data | 29 |
| Maternal — executive review | no data | no data | no data | no data | no data | no data | no data | no data | no data | no data | no data | 7 | 9 | 7 | 6 | 13 | 4 | 46 | no data | 8 |
| Maternal — full review | 10 | 12 | 4 | 15 | 8 | 21 | 11 | 3 | 3 | 11 | 3 | 5 | 4 | 3 | 9 | 8 | 8 | 138 | no data | 8 |
| Maternal — total | 10 | 12 | 4 | 15 | 8 | 21 | 11 | 3 | 3 | 11 | 3 | 12 | 13 | 10 | 15 | 21 | 12 | 184 | 38 | 11 |
| Neonatal | 12 | 11 | 13 | 12 | 12 | 16 | 19 | 14 | 20 | 10 | 5 | 15 | 10 | 8 | 10 | 11 | 8 | 206 | 42 | 12 |
| Stillbirth | 8 | 7 | 8 | 0 | 10 | 9 | 11 | 13 | 9 | 5 | 2 | 4 | 3 | 1 | 2 | 2 | 3 | 97 | 20 | 6 |
Chart One indicates that the total number of cases reviewed from 2004–2020 has varied from a low of 10 cases in 2014, to a high of 46 cases in 2009. This variance is likely reflective of committee administrative practices (e.g., time required for processing of review materials and compilation of final reports).
Graph one: Total number of cases reviewed by the MPDRC based on year (2004–2020)
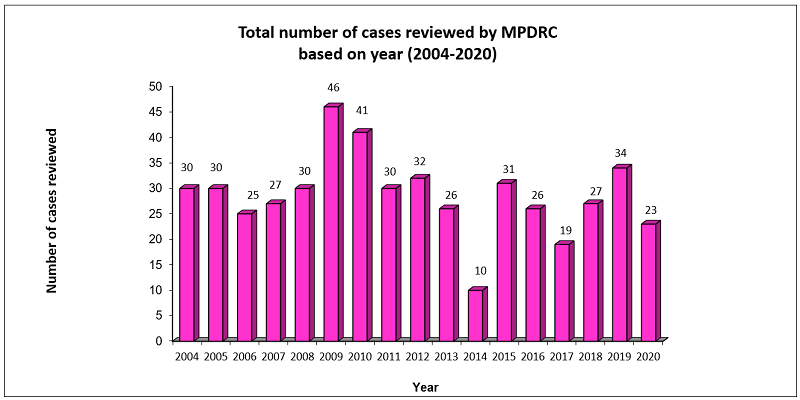
Graph One demonstrates how the number of cases reviewed from 2004–2020 from a low of 10 in 2014, to a high of 46 in 2009. This variance is due to the subjective nature of referrals to the committee (i.e., only maternal deaths result in mandatory referrals and all others are at the discretion of the regional supervising coroner) and administrative issues. On average, the MPDRC reviews 29 cases per year.
Graph two: Number of cases reviewed based on type of case (2004–2020)
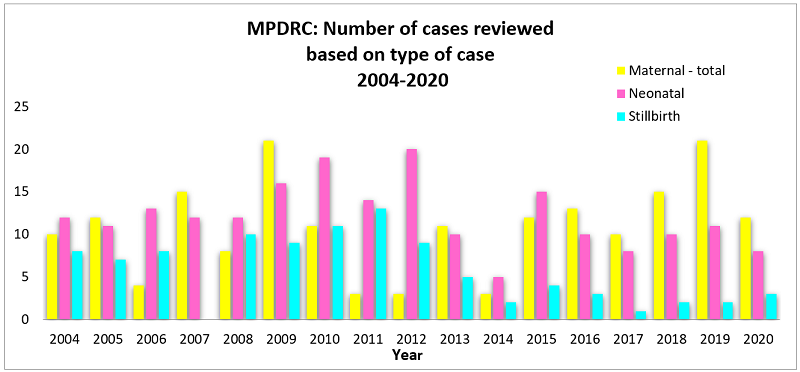
Graph Two demonstrates that, overall, from 2004–2020, the majority of cases reviewed are neonatal or maternal deaths. It is the policy of the Office of the Chief Coroner to review all maternal deaths in the province. Neonatal and stillbirth cases are reviewed when issues or concerns are identified.
Chart two: MPDRC — number of recommendations (2004–2020)
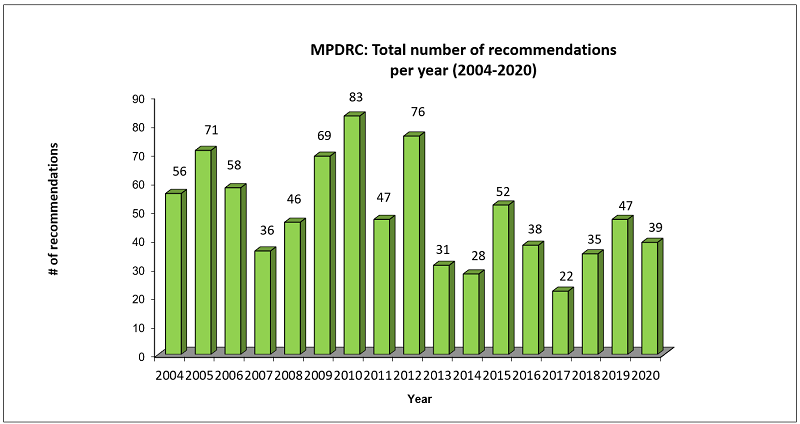
Chart Two indicates that the MPDRC has generated a total of 834 recommendations from 2004–2020. From this total, 174 (21%) were related to maternal cases, 462 (55%) from neonatal cases and 198 (24%) from stillbirth cases. Consistently over the years, the majority of cases and recommendations relate to reviews of neonatal deaths. On average, 49 recommendations are made per year.
Upon reviewing the recommendations that have been made, certain areas of concern have consistently emerged over time. The following general areas of concern have been identified:
- obstetrical care provider decisions
- policy and procedure (e.g., adherence or development of policy and procedures)
- communication/documentation (e.g., sharing and documenting information)
- quality (e.g., quality of care reviews)
- diagnosis and testing (e.g., interpretation of laboratory results)
- diagnosis and testing — specifically electronic fetal monitoring (EFM) (e.g., interpretation of results)
- education/training (e.g., continuing education)
- resources (e.g., access and allocation of resources)
- transfer (e.g., movement of patients)
- other (e.g., referral to another committee for review)
Graph three: Number of recommendations based on type of case 2004–2020
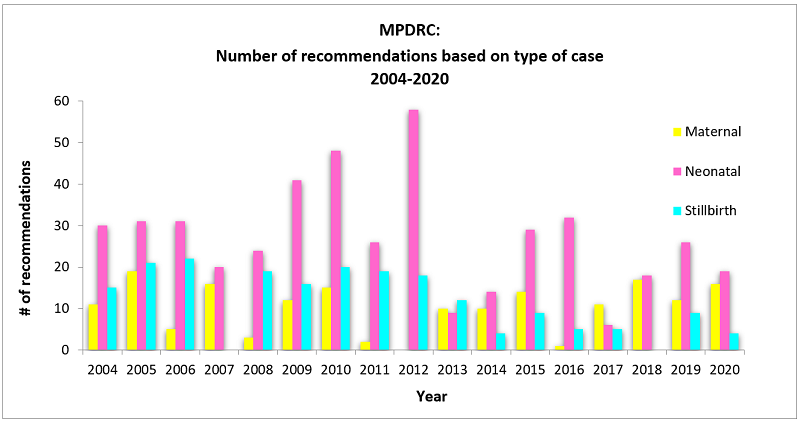
Graph Three demonstrates that from 2004–2020, most recommendations pertained to neonatal cases.
| Area of concern/theme | Maternal | Neonatal | Stillborn | Total | Percent of Total % |
|---|---|---|---|---|---|
| Obstetrical care provider | 69 37% |
89 18% |
47 23% |
205 | 23 |
| Policy and procedure | 33 18% |
88 18% |
35 17% |
156 | 18 |
| Communications/documentation | 18 10% |
80 16% |
37 18% |
135 | 15 |
| Quality of Care | 18 10% |
42 9% |
13 6% |
73 | 8 |
| Diagnosis and testing | 23 12% |
69 14% |
29 14% |
121 | 14 |
| Diagnosis and testing — EFM | 1 1% |
52 11% |
28 13% |
81 | 9 |
| Education/Training | 4 2% |
29 6% |
9 4% |
42 | 5 |
| Resources | 3 2% |
15 3% |
3 1% |
21 | 4 |
| Transfer | 8 4% |
19 4% |
5 2% |
32 | 4 |
| Other | 8 4% |
3 0.6% |
2 1% |
13 | 1 |
Note: Some recommendations touch on more than one theme.
Chart Three demonstrates that 23% of all recommendations made by the MPDRC from 2004–2020 relate to improving or addressing obstetrical care provider issues. An additional 18% of the recommendations pertain to the development of, or adherence to, policies and procedures and 15% to communication and/or documentation and in particular, the timely and accurate sharing of information between healthcare providers and with the patient.
Chart three also demonstrates the following key areas (based on type of case and theme):
- 18% of all recommendations from neonatal cases had an obstetrical care provider or policy and procedure theme, followed closely by 16% for communication and documentation
- 37% of all recommendations from maternal cases had the theme of obstetrical care provider (i.e., medical decisions)
- 23% of all recommendations from all cases had the theme of obstetrical care provider.
One area of specific concern that has been identified over the past few years relates to the use of electronic fetal monitoring (EFM) technology, how EFM results are interpreted by obstetrical care providers and what follow-up actions are taken in response to the findings. From 2004–2020, there have been 81 (9% of the total) recommendations made specifically pertaining to EFM.