2017 data on inmates in Ontario
Get 2017 data on inmate segregation, restrictive confinement and deaths in correctional facilities.
Review of all inmates on January 10, 2017, March 4, 2017 and June 1, 2017
The review identified all inmates admitted to a correctional facility on January 10, 2017, March 4, 2017 and June 1, 2017
On those days, there were a total of 462 inmates admitted on the three dates, excluding intermittent offenders, inmates already admitted at a facility but who had a change in status, and inmates transferred from another facility. This review examined whether and when various standard procedures — mental health screening, physician referrals, and mental health reassessments, for example — occurred for the identified inmates.
Inmates who were admitted on these dates were individually reviewed to determine whether and when a variety of required processes occurred, including:
- mental health screening upon admission
- reassessment using the mental health screening tools
For individuals who screened positive for possible mental health issues through mental health screening tools, the file review also looked at:
- whether a treatment plan was developed
- whether a physician assessed the inmate to determine if a referral to a psychiatrist was necessary
- whether a referral to a psychiatrist or other mental health care professional was made, when deemed necessary by a physician
Mental health screening and assessment
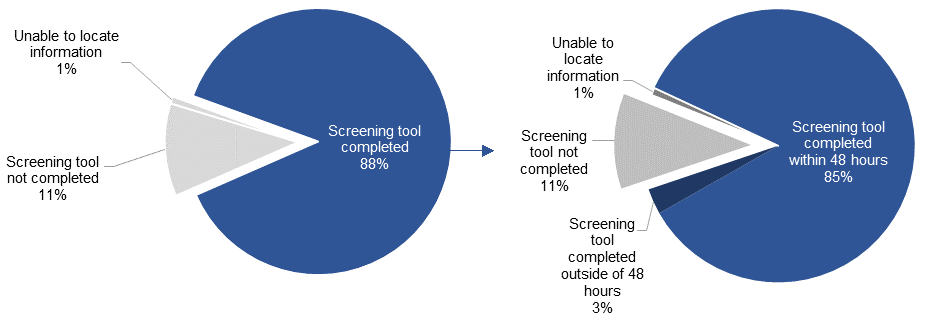
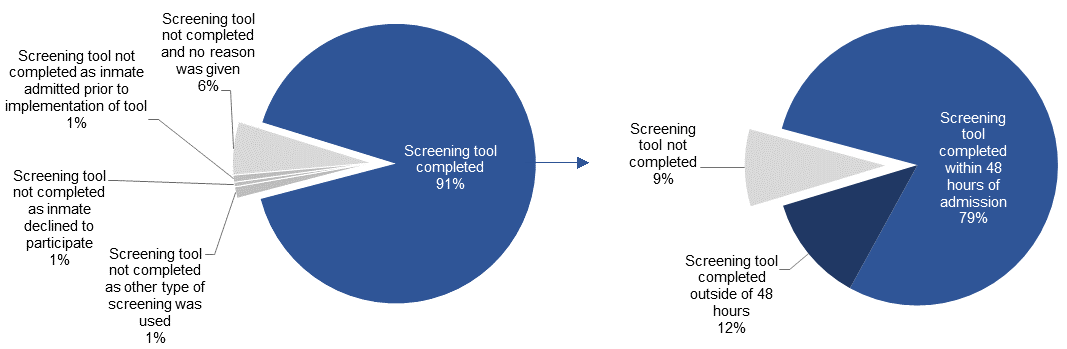
Ministry policy requires that initial mental health screening — which is completed using the Brief Jail Mental Health Screening Tool (BJMHS) — be conducted within 48 hours of an inmate being admitted to an institution. This tool is used to identify inmates with a possible mental illness. Those who are identified as having a possible mental illness receive a further, more in-depth assessment.
Of the 462 inmates covered in the review, 406 were administered the BJMHS, 52 were not completed and in four cases the information was not able to be found.
Of the 406 inmates who received the BJMHS, 392 had the assessment completed within 48 hours of admission and 14 were completed beyond 48 hours.
Rate of Brief Jail Mental Health Screening (BJMHS) Tool completion
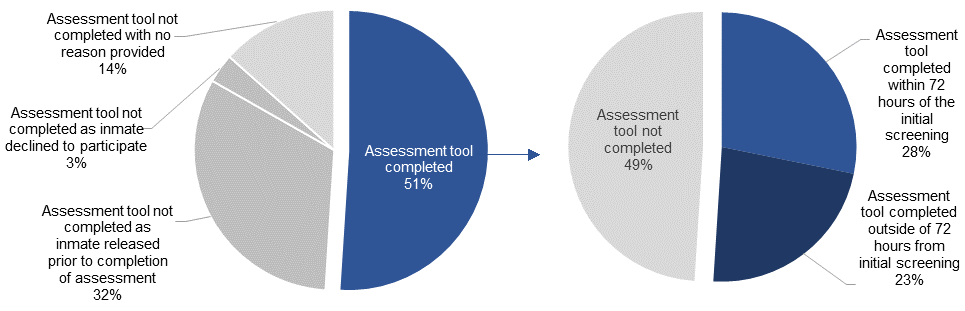
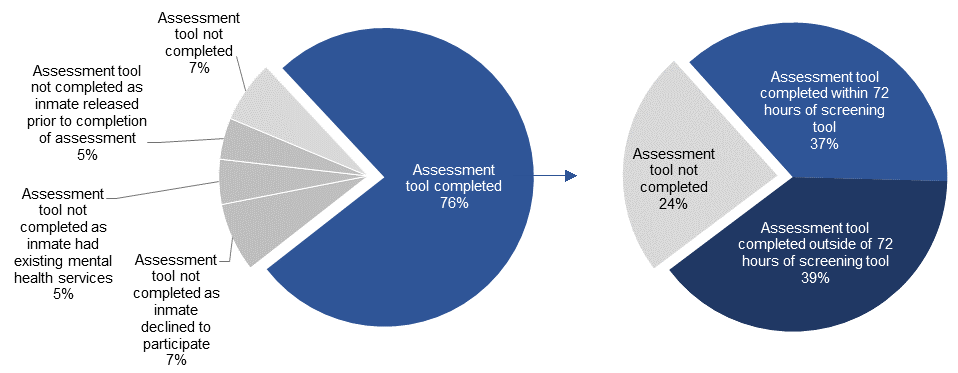
If a result on the initial screening tool is positive, ministry policy requires that a more comprehensive assessment — the Jail Screening Assessment Tool (JSAT) — be administered. The JSAT should be completed within 72 hours of the BJMHS. This assessment is completed by a mental health nurse, social worker or other trained mental healthcare professional to determine, based on the results of the assessment and their professional judgement, whether an inmate has a possible mental health disability.
Following the initial screening through the BJMHS, 149 inmates required further assessment using the JSAT and 76 were assessed using the tool. Of those who did not receive the JSAT assessment:
- 48 inmates were released prior to completion of the assessment
- five inmates declined to be assessed
- 20 inmates did not complete the screening and no reason was provided
Of the 76 inmates who were assessed, 42 had the assessment completed within 72 hours and 34 were completed outside of 72 hours. Of the 34 assessments that were completed outside of 72 hours, seven were completed within one week of admission and an additional 11 were completed within two weeks of admission.
Rate of Jail Screening Assessment Tool completion
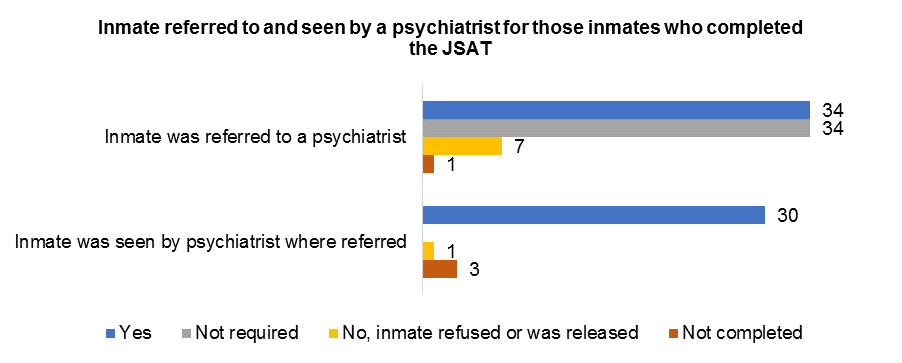
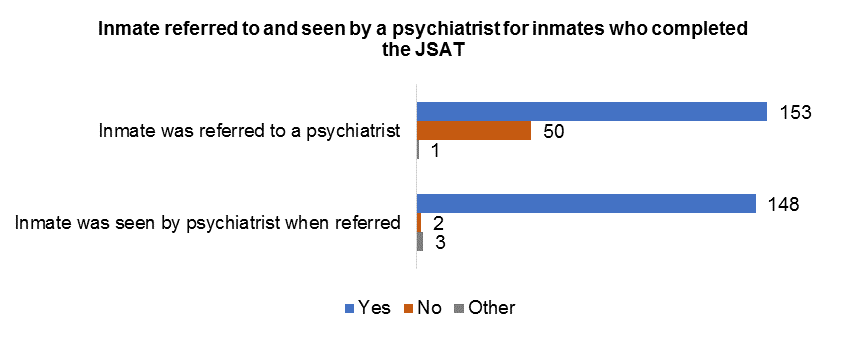
The review also examined whether inmates who screened positive for mental health disabilities through the JSAT were subsequently referred to a psychiatrist, and if the inmate was seen by a psychiatrist after being referred. Of the 76 inmates who were assessed using the JSAT, 34 were referred to see a psychiatrist and 30 of these inmates actually seen by a psychiatrist. Some inmates who had not yet completed the BJMHS and JSAT were seen by a psychiatrist outside of this process if they showed symptoms or had a history of a mental health disability. As a result, an additional 23 inmates who had not been screened using the JSAT were seen by a psychiatrist.
Mental health reassessment with screening tools
The review examined whether and when inmates were reassessed using the mental health screening tools the ministry uses when an inmate is admitted to a correctional institution – the BJMHS and JSAT. These tools, however, are not used for reassessment purposes. As a result, the inmates identified as part of the review were not reassessed using these tools.
Inmates with identified mental health disabilities are followed by mental health providers and seen on a regular basis. In general, however, inmates who are not identified as having a mental health care need through the BJMHS and JSAT screening are not being reassessed for mental health issues at regular intervals. For this population, reassessments occur when a member of the mental health care team is made aware that an inmate has shown significant behavioural change, when there are health or medication changes, or when it is court ordered. The ministry is developing a policy and a standardized tool to ensure all inmates are reassessed for mental health care needs at least once every 6 months. This policy will be in place and operational by July 31, 2018.
Treatment and care plans
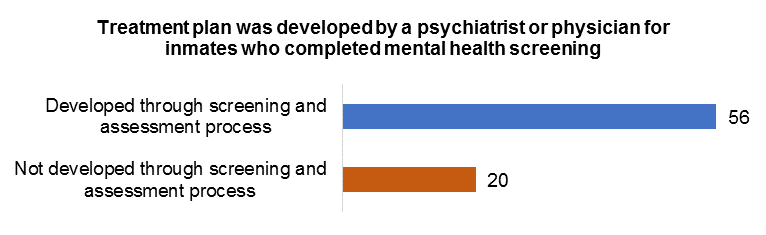
The point in time review tracked whether a treatment plan was developed by a physician or psychiatrist for inmates who were screened using the JSAT. A treatment plan outlines the medical strategies, ongoing services and treatment goals for a patient and, where appropriate, is developed with other mental health providers and clinical staff.
Fifty-six inmates who were assessed using the JSAT had a treatment plan developed. Treatment plans are not limited to those inmates screened through the JSAT. As a result, an additional 72 inmates had treatment plans on file.
Care plans may also be created for inmates in segregation with a mental health disability. Care plans are developed by a professional team that includes a combination of correctional staff, program staff, mental health providers, Indigenous inmate liaison officers, social workers, or community outreach workers. These plans ensure a consistent approach to support and meet the needs of an inmate. Of the 462 inmates included in the review, 24 inmates had a care plan developed.
The ministry recognizes the challenges of having multiple plans when caring for both the mental and physical health of an individual in custody. While it is important to share information, personal health information is considered confidential and subject to privacy provisions.
To balance the privacy rights of individuals and the importance of sharing critical information with all staff providing oversight and care, the ministry will be examining options for a more comprehensive, multidisciplinary care plan with the goal of enhancing information sharing while supporting approaches to treatment.
This will be in consultation with mental health professionals, the OHRC, community stakeholders and the Independent Expert on Human Rights and Corrections.
Review of all inmate admissions on November 1, 2017
The review identified all inmates admitted to a correctional facility on November 1, 2017 at six institutions identified by the OHRC. These institutions were:
- Central East Correctional Centre
- Kenora Jail
- Niagara Detention Centre
- North Bay Jail
- Ottawa-Carleton Detention Centre
- Vanier Centre for Women
There were a total of 37 inmates admitted on the date, excluding intermittent offenders, inmates already admitted at a facility but who had a change in status and inmates transferred from another facility. This review examined whether and when various standard procedures occurred for the identified inmates.
Inmates who were admitted on November 1 had individual reviews of their files to determine whether and when a variety of required processes occurred, including:
- initial mental health screening upon admission
- further assessment when indicated by the initial screening tool
- reassessment within six months of admission
For individuals who screened positive for possible mental health issues through the mental health screening and assessment tools, the file review also considered whether and when:
- a physician assessed the inmate to determine if a referral to a psychiatrist was necessary
- a referral to a psychiatrist or other mental health care professional was made, when deemed necessary by a physician
- the inmate was seen by the psychiatrist or other mental health care professional where referred
- a treatment plan was developed
Of the 37 inmates included in the review, 10 identified as female and 27 as male. No inmates captured in this review identified as transgender. Upon admission nine women and 22 men were being held on remand, one woman was admitted as a police lock-up and five men were admitted to serve a sentence. As of June 12, 2018, the average length of stay for inmates covered in this review was 36 days for women and 55 days for men.
Mental health screening and assessment
Brief Jail Mental Health Screening tool
Ministry policy requires that initial mental health screening, which is completed using the Brief Jail Mental Health Screening (BJMHS) tool, be conducted within 48 hours of an inmate being admitted to an institution. This tool is used to identify inmates with a possible mental illness. Those who are identified as having a possible mental illness receive a further, more in-depth assessment.
Of the 37 inmates covered in the review, 36 were administered the BJMHS. The one inmate who did not receive the BJMHS, was admitted after hours and released the following morning at court.
Of the 36 inmates who received the BJMHS, all had the assessment completed within 48 hours of admission.
Jail Screening Assessment Tool
If a result on the initial screening tool is positive, ministry policy requires that a more comprehensive assessment, the Jail Screening Assessment Tool (JSAT), be administered. Ministry policy also requires that the JSAT is completed within 72 hours of the BJMHS. This assessment is completed by a mental health nurse, social worker or other trained mental healthcare professional to determine, based on the results of the assessment and their professional judgement, whether an inmate has a possible mental health condition.
Following the initial screening through the BJMHS, 15 inmates required further assessment using the JSAT and nine were assessed using the tool. The remaining six inmates who required but did not receive the JSAT assessment were released before the assessment could be completed.
Of the nine inmates who were assessed, eight had the assessment completed within 72 hours and one was completed outside of 72 hours.
Referrals to physicians and psychiatrists
The review also examined whether inmates who screened positive for mental health conditions through the JSAT were subsequently referred to a psychiatrist, and if the inmate was seen by a psychiatrist after being referred. Of the nine inmates who were assessed using the JSAT, two were referred to a physician, one of whom was referred to a psychiatrist for further assessment.
Some inmates were seen by a psychiatrist or other mental health professional outside of the above screening process if they showed symptoms or had a history of a mental health condition. As a result, an additional five inmates were seen by a psychiatrist.
Mental health reassessment
The review examined whether and when inmates were reassessed using the BJMHS and JSAT mental health screening tools the ministry uses when an inmate is admitted to a correctional institution. These tools, however, are not designed for reassessment purposes. As a result, the inmates identified as part of the review were not reassessed using these tools. However, the review captured that 25 of the 37 inmates were released before six months and of the remaining 12 inmates, 11 were reassessed within six months of admission.
Inmates with identified mental health conditions are followed by mental health providers and seen on a regular basis. In general, however, inmates who are not identified as having a mental health care need through the BJMHS and JSAT screening, are not being reassessed for mental health issues at regular intervals. For these inmates, reassessments occur when a member of the mental health care team is made aware that:
- an inmate has shown significant behavioural change
- there are health or medication changes
- a reassessment is court ordered
The ministry has implemented a new health care policy for reassessing inmates within six months of admission. This policy and a newly developed tool was rolled out at all institutions on July 31, 2018 and will be reviewed for compliance in March 2019.
Treatment and care plans
The point-in-time review tracked whether a treatment plan was developed by a physician or psychiatrist for inmates who were screened using the JSAT. A treatment plan may address any physical or mental health concerns and may include medical strategies, ongoing services and treatment goals for a patient. Where appropriate, a treatment plan is developed with other mental health providers and clinical staff.
| Was a treatment plan developed? | Number of female inmates | Number of male inmates | Total number of inmates |
|---|---|---|---|
| Yes, developed following referral to mental health professional | 1 | 3 | 4 |
| Existing treatment plan already in place | 2 | 8 | 10 |
| Not developed or required | 7 | 16 | 23 |
| Total number of inmates | 10 | 27 | 37 |
Six inmates who were assessed using the JSAT had a treatment plan developed. Three of these treatment plans were in place prior to the mental health screening. Treatment plans are not limited to those inmates screened through the JSAT. As a result, an additional eight inmates, for a total of 14, had treatment plans developed or already on file from a previous admission.
To guide goals of care and support inmates’ needs, including health concerns, care plans may also be developed, but are not required. Care plans are collaboratively written documents developed by a professional team including a combination of:
- correctional staff
- program staff
- mental health providers
- Indigenous inmate liaison officers
- social workers
- community outreach workers
| Does the inmate have a care plan? | Number of female inmates | Number of male inmates | Total number of inmates |
|---|---|---|---|
| Yes | n/a | 4 | 4 |
| No | 10 | 23 | 33 |
| Total number of inmates | 10 | 27 | 37 |
Of the 37 inmates covered in the review, a total of four had care plans. Of these four, two had been flagged by the screening process. It is unknown as to whether the care plans relate back to an underlying mental illness or condition.
The ministry recognizes the challenges of using multiple plans to address an individual’s mental and physical health needs. While it is important to share information, personal health information is considered confidential and subject to privacy provisions. To balance the privacy rights of individuals and the importance of sharing critical information with all staff providing oversight and care, the ministry is examining options for a more comprehensive, multidisciplinary care plan with the goal of enhancing information sharing while supporting approaches to treatment. This will be in consultation with mental health professionals, the OHRC, community stakeholders and the Independent Expert on Human Rights and Corrections.
Review of inmates with possible mental health conditions who were in segregation on November 14, 2017
The review identified all individuals with possible mental health disabilities in segregation on November 14, 2017.
On that day, 609 inmates were identified as being in segregation. The determination of which inmates were in segregation was made based on current ministry policy, which requires that institutions designate specific cells or units as segregation. Inmates housed in other types of specialized units — including special needs units, special handling units, mental health units, or behavioral units — were not classified as being placed in segregation.
Of the 609 segregated inmates, 373 were identified as having possible mental health disabilities. The identification of inmates with possible mental health disabilities was based on:
- an active mental health alert
- results of the ministry’s standard mental health screening and assessment tools
- information that was reported and confirmed by a healthcare professional
These 373 inmates’ files were individually reviewed to determine whether and when a variety of required processes occurred, including:
- mental health screening upon admission
- reassessment using the mental health screening tools
- consideration of alternatives to the point of undue hardship prior to the segregation placement
- baseline and ongoing five-day health assessments by a physician or psychiatrist upon placement in segregation
For individuals who screened positive for possible mental health issues through mental health screening tools, the file review also looked at whether and when:
- a treatment plan was developed
- a physician assessed the inmate to determine if a referral to a psychiatrist was necessary
- a referral to a psychiatrist or other mental health care professional was made, when deemed necessary by a physician
Finally, the review considered whether segregation reviews and reports were appropriately completed, including:
- the completion of five-day and 30-day segregation reviews, including documentation of the alternatives that were considered and rejected and whether a treatment plan was in place
- whether 30-day segregation reports were prepared and received by the minister, and whether the reports documented:
- alternatives that were considered and rejected
- whether a treatment plan was in place
- whether the individual had a mental illness
- whether a 60-day aggregate segregation report were prepared and received by the Assistant Deputy Minister, Institutional Services, and whether these reports documented when an individual had a mental illness
| Institution | Total number of inmates in custody on November 14, 2017 | Number of inmates in segregation with possible mental health disabilities on November 14, 2017 |
|---|---|---|
| Brantford Jail | 63 | 2 |
| Elgin-Middlesex Detention Centre | 379 | 11 |
| Hamilton-Wentworth Detention Centre | 459 | 12 |
| Niagara Detention Centre | 200 | 15 |
| Sarnia Jail | 34 | 2 |
| Southwest Detention Centre | 275 | 8 |
| Brockville Jail | 21 | 3 |
| Central East Correctional Centre | 956 | 92 |
| Ottawa-Carleton Detention Centre | 385 | 33 |
| Quinte Detention Centre | 197 | 16 |
| St. Lawrence Valley Centre | 97 | 2 |
| Central North Correctional Centre | 788 | 59 |
| Kenora Jail | 139 | 3 |
| Monteith Correctional Complex | 90 | 2 |
| North Bay Jail | 69 | 5 |
| Sudbury Jail | 117 | 10 |
| Thunder Bay Correctional Centre | 74 | 1 |
| Thunder Bay Jail | 127 | 1 |
| Maplehurst Correctional Complex | 1,031 | 52 |
| Ontario Correctional Institute | 128 | 1 |
| Toronto East Detention Centre | 389 | 4 |
| Toronto South Detention Centre | 879 | 14 |
| Vanier Centre for Women | 207 | 25 |
Mental health screening and assessments
Ministry policy requires that initial mental health screening – which is completed using the Brief Jail Mental Health Screening Tool (BJMHS) – be conducted within 48 hours of an inmate being admitted to an institution. This tool is used to identify inmates with a possible mental illness. Those who are identified as having a possible mental illness receive a further, more in-depth assessment.
Of the 373 inmates covered in the review, 340 were administered the BJMHS. Of the inmates who did not have the BJMHS screening:
- the screening tool was not completed for 23 inmates with no reason indicated
- in three instances, the screening tool was not completed as the inmates were admitted prior to the implementation of the tool
- for one inmate, the screening tool was not completed as another type of screening was used
- in four cases, the assessment tool was not completed as the inmates were already receiving mental health services
- the screening tool was not completed for two inmates as the inmate declined to participate
Of the 340 inmates who received the BJMHS, 294 had the assessment completed within 48 hours of admission and 44 were completed beyond 48 hours.
Brief Jail Mental Health Screening (BJMHS) Tool Completion
If a result on the initial screening tool indicates a mental health concern, ministry policy requires that a more comprehensive assessment – the Jail Screening Assessment Tool (JSAT) – be administered. Unless a JSAT has been administered in a prior term of incarceration, in which case the prior assessment can be relied upon, the inmate should receive a JSAT assessment within 72 hours of the BJMHS. This assessment is completed by a mental health nurse, social worker or other trained mental healthcare professional to determine, based on the results of the assessment and their professional judgement, whether an inmate has a possible mental health disability.
Following the initial screening through the BJMHS, 267 inmates required further assessment using the JSAT and 204 were assessed using the tool. Of those who did not receive the JSAT assessment:
- in 13 cases, the assessment tool was not completed as the inmates were already receiving mental health services
- the assessment tool was not completed for 12 inmates as the inmates were released prior to completion of the assessment
- for 20 inmates, the assessment tool was not completed as the inmate declined to participate
- in 18 cases, the assessment tool was not completed and no reason was provided
Of the 204 inmates who were assessed, 99 had the assessment completed within 72 hours and 92 were completed outside of 72 hours. Eight inmates had an assessment completed during a prior admission to custody and in five cases, the date of the assessment was unable to be determined.
Of the 92 assessments that were completed beyond 72 hours, 27 were completed within one week of admission and an additional 17 were completed within two weeks of admission.
Jail Screening Assessment Tool Completion
The review also examined whether inmates who screened positive for possible mental health disabilities through the JSAT were subsequently referred to a psychiatrist, and if the inmate was seen by a psychiatrist after being referred. Some inmates were seen by a psychiatrist outside of this process if they showed symptoms or had a history of a mental health disability. As a result, the total number of inmates seen by a psychiatrist was higher than the number referred to a psychiatrist through the JSAT assessment process.
One hundred fifty-three out of the 204 inmates who received a JSAT assessment were referred to a psychiatrist. Of the 153 who were referred, 148 were seen by a psychiatrist. An additional 119 inmates were seen by a psychiatrist outside of the BJMHS and JSAT referral process.
In cases where a psychiatrist is unavailable, inmates may be seen by clinical staff or a mental health provider such as a psychologist, mental health nurse, social worker, or psychometrist. However, consultations with a psychiatrist still occur as soon as possible, and based on urgency.
Mental health reassessments using the mental health screening tools
The review examined whether and when inmates were reassessed using the mental health screening tools the ministry uses when an inmate is admitted to a correctional institution – the BJMHS and JSAT. These tools, however, are not used for reassessment purposes. As a result, the inmates identified as part of the review were not reassessed using these tools.
Inmates with identified mental health disabilities are followed by mental health providers and seen on a regular basis. In general, however, inmates who are not identified as having a mental health care need through the BJMHS and JSAT screening are not being reassessed for mental health issues at regular intervals. For this population, reassessments occur when a member of the mental health care team is made aware that an inmate has shown significant behavioural change, when there are health or medication changes, or when it is court ordered. The ministry is developing a policy and a standardized tool to ensure all inmates are reassessed for mental health care needs at least once every 6 months. This policy will be in place and operational by July 31, 2018.
Ministry policy requires that all inmates in segregation be seen daily by healthcare staff. All inmates with a mental illness who are placed in segregation must also be regularly assessed by a mental health care provider.
Treatment and care plans
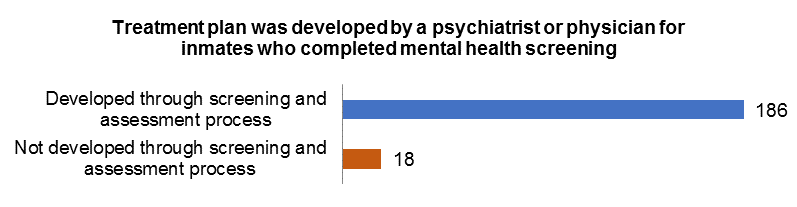
The point in time review tracked whether a treatment plan was developed by a physician or psychiatrist for inmates who were screened using the JSAT. A treatment plan outlines the medical strategies, ongoing services and treatment goals for a patient and, where appropriate, is developed with other mental health providers and clinical staff.
One hundred eighty-six inmates who were assessed using the JSAT had a treatment plan developed. Treatment plans are not limited to those inmates screened through the JSAT. As a result, an additional 115 inmates had treatment plans on file.
Care plans may also be created for segregated inmates who have a mental health disability. Care plans are developed by a professional team that includes a combination of correctional staff, program staff, mental health providers, Indigenous inmate liaison officers, social workers, or community outreach workers. These plans ensure a consistent approach to support, and to meet the individualized needs of an inmate. Overall, 188 of the 373 identified inmates had care plans on file.
The ministry recognizes the challenges of having multiple plans when caring for both the mental and physical health of an individual in custody. While it is important to share information, personal health information is considered confidential and subject to privacy provisions.
To balance the privacy rights of individuals and the importance of sharing critical information with all staff providing oversight and care, the ministry will be examining options for a more comprehensive, multidisciplinary care plan with the goal of enhancing information sharing while supporting approaches to treatment.
This will be in consultation with mental health professionals, the OHRC, community stakeholders and the Independent Expert on Human Rights and Corrections.
Baseline health assessments
When an inmate with a mental health disability is placed into segregation, a physician must offer the inmate a baseline health assessment. For inmates with major mental illness, this baseline assessment must be provided by a psychiatrist. Ministry policy requires that physicians or psychiatrists conduct this baseline assessment as soon as possible upon admission to segregation, to evaluate the treatment and care requirements of an inmate.
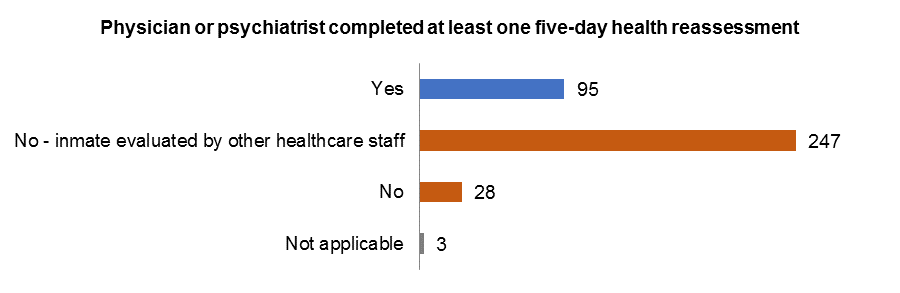
Inmates are to be reassessed by a physician or psychiatrist every five days following their original assessment. After an inmate is in segregation for five consecutive days – and prior to each subsequent five-day review of an inmate’s placement – ministry policy requires that a physician or psychiatrist complete a reassessment to determine if any changes are required to an inmate’s treatment plan.
In practice, due to the limited availability of physicians and psychiatrists, many facilities utilize other health care professionals – such as registered nurses or nurse practitioners – to perform the assessments.
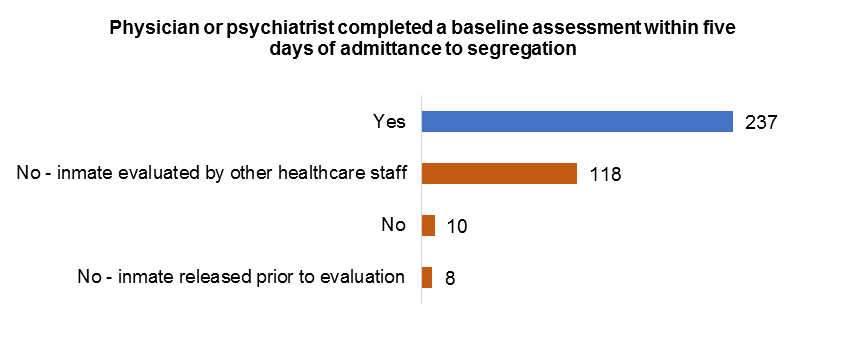
Results of the review demonstrate that subsequent five-day reassessments were primarily done by a healthcare professional other than a physician or psychiatrist.
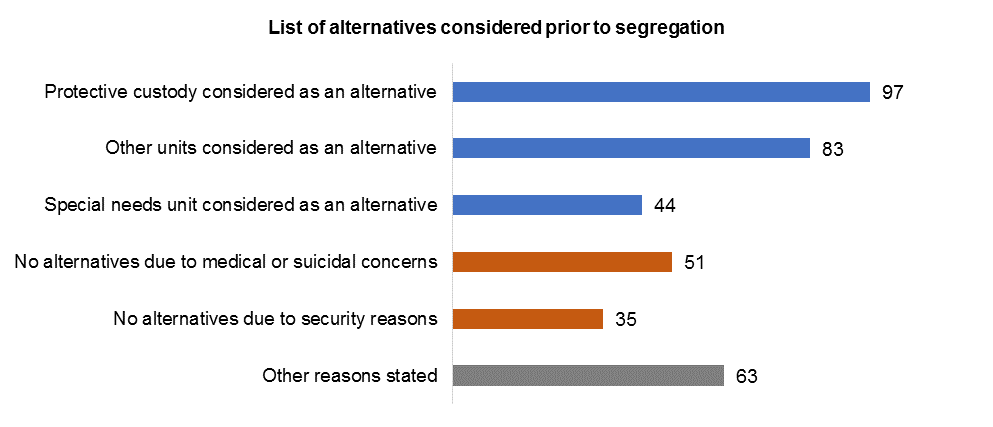
Consideration of alternatives to segregation
As part of the review, correctional institutions were required to report whether alternatives were considered to the point of undue hardship prior to an inmate being segregated. Ministry policy states that segregation may only be considered if an inmate:
- is in need of protection
- has requested to be segregated
- poses a security or safety risk to others
- is under medical observation or isolation
- has committed alleged misconduct
- requires confinement following misconduct
The review shows that alternatives were not always considered prior to an inmate’s initial segregation placement. If an inmate’s placement in segregation was a result of a significant disturbance, serious or violent misconduct, or recommended by a healthcare professional, the review results suggest that staff frequently determined that there were no immediate alternative options before authorizing the initial segregation placement.
Ministry policy requires that inmates who continue to be detained in segregation are subject to further case reviews, during which alternatives to segregation must be considered to the point of undue hardship.
Unfortunately, the methodology of this point in time review – that relied on manual compilation of information in paper files – did not allow for a detailed analysis of whether the undue hardship threshold was reached in each case. The information documented in the paper files is not necessarily an exhaustive list of all of the alternatives considered, and may not provide reasons as to why certain alternatives were not considered. The ministry will be working closely with the OHRC and an independent expert on human rights and corrections in future reviews to better articulate the components of the undue hardship analysis.
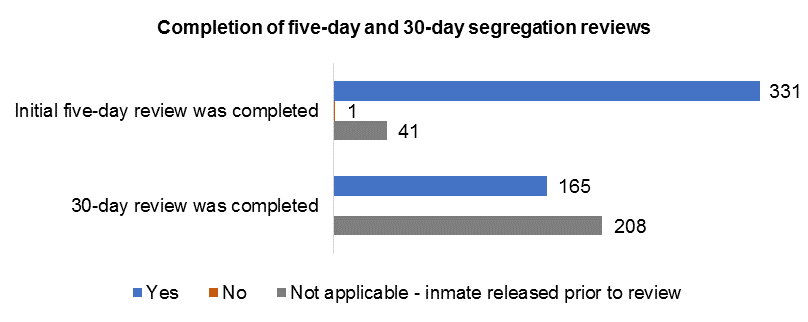
Completion of required segregation reviews
Ministry policy requires that inmates placed in segregation be reviewed within 24 hours, and every five days thereafter. Inmates who have been in segregation for 30 days or more must have their placement reviewed by the superintendent and the regional director in order for the inmate to continue in segregation. Treatment plans and alternatives to segregation considered to the point of undue hardship must be documented as part of the review process.
The data showed that all but one of the inmates had all of their required reviews completed.
Content and receipt of 30-day and 60-day segregation reports
Each month, reports are generated at the institutional and regional levels documenting the inmates who have been in segregation for more than 30 continuous days. These reports include:
- whether an inmate has a mental health alert
- a list of alternatives to segregation considered for each inmate
- whether each inmate has a treatment plan in place
Prior to February 15, 2018, these reports were provided to the assistant deputy minister, the deputy minister, and the minister in a summarized format, without the details listed above.
Inmates who have been in segregation for a combined total of more than 60 aggregate days within the last year are also included in a separate monthly report to the Assistant Deputy Minister of Institutional Services. These reports similarly did not document the individualized level of detail included in the institutional and regional segregation reports.
As of February 15, 2018, reports of inmates in segregation for 30 continuous days that are provided directly to the assistant deputy minister, the deputy minister, and the minister include additional details about the circumstances of each individual’s segregation placement and the alternatives to segregation considered. This level of detail also applies to the 60-day aggregate reports that are provided to the Assistant Deputy Minister of Institutional Services.