Paediatric Death Review Committee: medical
The Paediatric Death Review Committee (PDRC) – medical is a multi-disciplinary committee that consists of specialized paediatric practitioners including: paediatric pathology, paediatric critical care, community paediatrics, paediatric emergency medicine, neonatology and cardiology. The membership is balanced to reflect Ontario’s geography and includes differing levels of institutions that provide paediatric care and teaching centres, when possible.
Medical reviewers analyze and consider the medical issues involved in the time preceding a child’s death to gain a better understanding of the circumstances of the death. Case referrals for committee evaluation include medically complex deaths when there are concerns regarding the medical care or if there are questions about the clinical diagnosis, cause and/or manner of death.
Review process
Case assignment occurs by aligning the practice profile and expertise of the committee members with the circumstances of the death. For example, paediatric deaths from a community setting will be reviewed by one of the community paediatricians. Similarly, the death of a neonate will be primarily reviewed by the neonatologist. The review process involves analyzing the existing record of the decedent. The record routinely includes medical records, the Coroner’s Investigation Statement, the report of the post mortem examination, toxicology report, police report and other relevant documents.
At the committee meetings, the primary reviewer presents the findings to the members for discussion. This provides an opportunity for discussion about issues that may have been identified through the review. The committee may also develop recommendations based on the findings of the review. The primary reviewer will compose a final report reflecting the committee’s consensus opinion. The report, which will include the cause and manner of death and any committee recommendations, is provided to the referring Regional Supervising Coroner. If the recommendations are systemic, the ministry, organization, agency or individuals are notified by the Committee Chair. Organizations were asked to respond back with the status of implementing the recommendation(s) within one year. Commencing in 2017, organizations were asked to respond back within six months of receiving the recommendations, which is consistent with the approach to inquest recommendations.
Where a case presents a potential or real conflict of interest for a committee member, that member will not participate in the review. Should a case require expertise from another discipline, an external expert will review and attend a PDRC meeting to participate in the discussion and drafting of recommendations.
Limitations
The PDRC case reports are prepared for the OCC and are governed by the Coroners Act, the Vital Statistics Act, the Freedom of Information and Protection of Privacy Act and the Personal Health Information and Protection of Privacy Act.
The consensus report of the committee is limited by the data provided. While efforts are made to obtain all relevant data, it is important to acknowledge that these reports are generated from a review of the written records. Sometimes the coroner/Regional Supervising Coroner conducting the investigation may have received additional information not included in the records that may render one or more of the committee's conclusions invalid.
Recommendations are made following a careful review of the circumstances of each death; they are not intended to be policy directives.
Statistical analysis for Paediatric Death Review Committee – medical
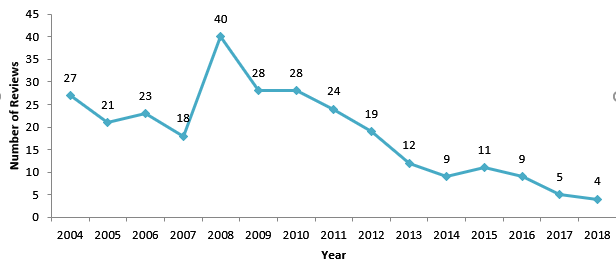
The number of PDRC – medical reviews varies from year to year. Chart 12 illustrates the number of PDRC - Medical reviews from 2004 to 2018. In 2018, there were four cases reviewed.
Chart 12: PDRC (medical) – Total number of reviews (2004-2018)