Appendices
Appendix A: Family Profiles
The following three scenarios demonstrate the type of needs that might lead a family to request or be referred to Coordinated Service Planning. They also demonstrate how different family circumstances could result in families receiving different intensities of service and less or more frequent contact with their Service Planning Coordinator.
Sample Profile 1:
A 15-year-old youth, diagnosed with Autism Spectrum Disorder when he was young, has been accessing multiple services and supports for many years, including mental health, autism, and behavioural services, respite and educational supports. The current service providers work well together, but there is no Coordinated Service Plan. Lately, his aggressive behavior has increased, and both his parents and the school are struggling with managing his behaviours and keeping other children safe from his aggressive outbursts.
Sample Profile 2:
An 8 year old, diagnosed with Dystonic Cerebral Palsy and Chronic Lung Disease (oxygen dependent) has also been diagnosed with Global Developmental delays. She was born at almost 29 weeks gestation and developed neonatal meningitis.
She is frequently hospitalized for pneumonia, usually in intensive care and has required intubation during some of those hospitalizations. Both parents are involved in her care but don’t live together. She resides with her mother and an older sister. She requires hands-on care for feeding and other daily living activities and receives nightly nursing care. School attendance is sporadic due to her medical needs but when she does attend she receives assistance from an Educational Assistant and a Nurse. The youth receives 8 days of respite per month in the community.
Sample Profile 3:
An 18-month old has just been identified by a pediatrician as having delays in speech and language, social and motor development. The parent is a single parent with 3-year-old twins.
Note: The child and family in Sample Profile 3 may or may not receive Coordinated Service Planning, depending on other circumstances in their lives. Because their case is less complex, they may receive less intensive Coordinated Service Planning or a warm referral to other services with an invitation to return to the Coordinating Agency if their circumstances become more complex.
Appendix B: Map of Service Delivery Areas
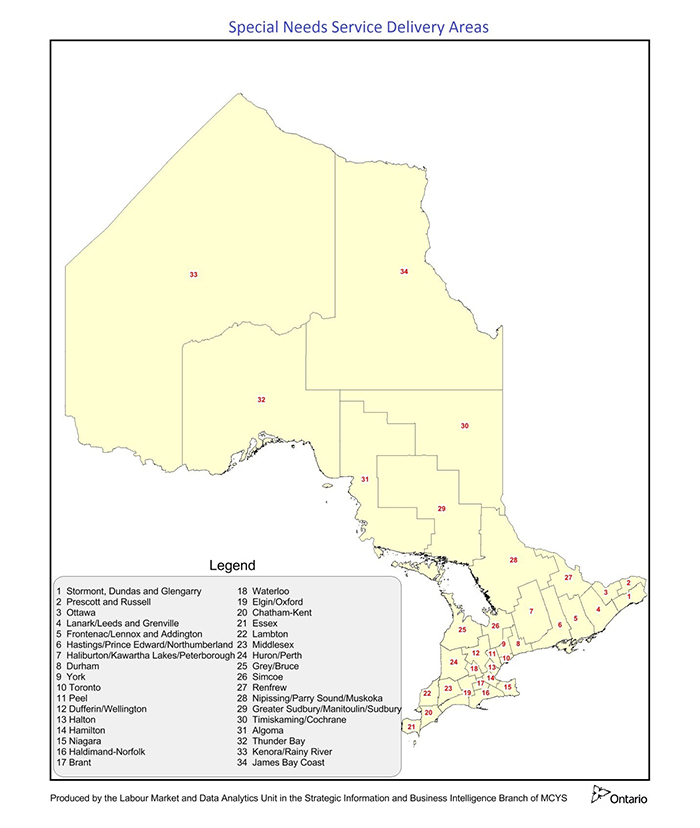
Special Needs Service Delivery Areas
Legend
- Stormont, Dundas et Gengarry
- Prescott et Russell
- Ottawa
- Lanark/Leeds et Grenville
- Frontenac/Lennox et Addington
- Hastings/Prince Edward/Northumberland
- Haliburton/Kawartha Lakes/Peterborough
- Durham
- York
- Toronto
- Peel
- Dufferin/Wellington
- Halton
- Hamilton
- Niagara
- Haldimand-Norfolk
- Brant
- Waterloo
- Elgin/Oxford
- Chatham-Kent
- Essex
- Lambton
- Midddlesex
- Huron/Perth
- Grey/Bruce
- Simcoe
- Renfrew
- Nipissing/Parry Sound/Muskoka
- Greater Sudbury/Manitoulin/Sudbury
- Timiskaming/Cochrane
- Algoma
- Thunder Bay
- Kenora/Rainy River
- Côte de la baie James
Produced by the Labour Market and Data Analytics Unit in the Strategic Information and Business Intelligence Branch of MCCSS.
Appendix C: Roles and Responsibilities in the Integrated Transition Planning Process
Coordinating Agencies have specific responsibility to initiate the integrated transition process implemented by the Ministries of Children, Community and Social Services, and Education. This process connects closely with Individual Education Plan (IEP) processes and adult services. Outlined below are the roles and responsibilities for the parties involved in the development of an integrated transition plan for a young person with developmental disabilities who also has a Coordinated Service Plan:
Roles and Responsibilities in the Integrated Transition Planning Process
Service Planning Coordinator
- Identify individuals with in their 14th year (and up) who have a Coordinated Service Plan and require a single integrated transition plan.
- Provide information to the parent/young person about integrated transition planning.
- When the young person is about to turn 14, ask the parent/young person if they would like an integrated transition plan.
- Identify and contact the school IEP lead (as designated by the principal) to begin the integrated transition planning process that leads to a single integrated transition plan as part of the IEP process.
- Identify and contact relevant children’s services providers to participate as part of the integrated transition planning team.
- Identify and contact the young person’s Community Care Access Centre (CCAC) case manager (if applicable) to participate as part of the integrated transition planning team.
- Identify other relevant health service providers and invite them to participate as part of the integrated transition planning team.
- Ensure that the proper consents are received from the young person with multiple and/or complex special needs and their parent/guardian in the integrated transition planning process.
- Seek to ensure that all parties understand and are in agreement with the integrated transition plan and have all the information they require, including any accessibility-related requirements/modifications that should be provided to the school.
- Participate, as required, in meetings regarding the single integrated transition plan which identifies the young person’s health care needs, goals for work, further education, employability skills and community living.
- Working with the school IEP lead, support the young person and their parent/guardian to participate throughout the integrated planning process.
- Incorporate the single integrated transition plan as provided by the school IEP lead to the parents (and student if 16 and older) into the Coordinated Service Plan.
- Lead the ongoing review, and, with the young person, family, and integrated transition planning team, and update the integrated transition plan at regular intervals or as needed.
- Provide a copy of the Coordinated Service Plan, which includes the single integrated transition plan, to all relevant parties, including the parent (and student if 16 and older).
Schools
- Begin integrated transition planning at age 14 as part of the IEP process. The school IEP lead is designated by the principal.
- Establish, participate in and contribute to integrated transition planning teams.
- Working with the Service Planning Coordinator, provide opportunities for the individual and their parent or guardian to participate throughout the integrated transition planning process.
- Establish a process for the school IEP lead to contact/link with designated community agency staff person to begin the integrated transition planning process, if appropriate.
- Ensure that the proper consents are received from the young person with multiple and/or complex special needs and his/her parent/guardian to initiate the integrated transition planning process.
- Provide information to the family/young person regarding application to the DSO, if applicable.
- Provide a copy of the IEP, which includes the single integrated transition plan, to the parents (and student if 16 and older) and include a copy in the student’s Ontario Student Record (OSR).
- Establish a process for the single integrated transition plan to be reviewed and updated as required.
Children’s Services Providers
- Participate in, and contribute to the integrated transition planning team.
Health Service Providers (e.g. primary care, Local Health Integration Networks, Community Care Access Centres)
- Participate in, and contribute to the integrated transition planning team.
Developmental Services Ontario (DSO) Organizations
- The DSO is the primary point of contact for public inquiries about MCCSS-funded adult developmental services and supports for persons with developmental disabilities in accordance with the Services and Supports to Promote the Social Inclusion of Persons with Developmental Disabilities Act, 2008 (SIPDDA).
- DSO will also provide a single point of access for persons with developmental disabilities to MCCSS-funded adult developmental services and supports in Ontario.
- Upon request, the DSO organization will provide information to the integrated transition planning team or to the school / school board on the services and supports that may be provided by community agencies in its geographic service area.
- They will employ qualified assessors to administer the Application Package with each eligible applicant to assess support needs. The Application Package comprises the Application for Developmental Services and Supports (ADSS) and the Supports Intensity Scale® (SIS®).
- Qualified assessors may administer the Application Package with applicants from the age of sixteen who, with the exception of the age requirement, meet the criteria for MCCSS-funded adult developmental services and supports in accordance with the Act.
- Provide the Service Planning Coordinator with a contact/link with person-directed planners/facilitators in the community where available, to continue the integrated transition planning process for individuals with complex care needs until the transition to adult services.
- A representative from a DSO and/or adult DS agency will be available to provide information to integrated transition planning teams about eligibility criteria, the application process and relevant community-based services for adults with a developmental disability. They will also be available to provide advice on elements that should be considered as part of planning transitions to adulthood and they can attend transition planning meetings as required.