Part 4: The Coordinated Service Planning Cycle
Coordinating Agencies are expected to work with their partners to provide the following, in a clear and consistent way:
Text version of infographic
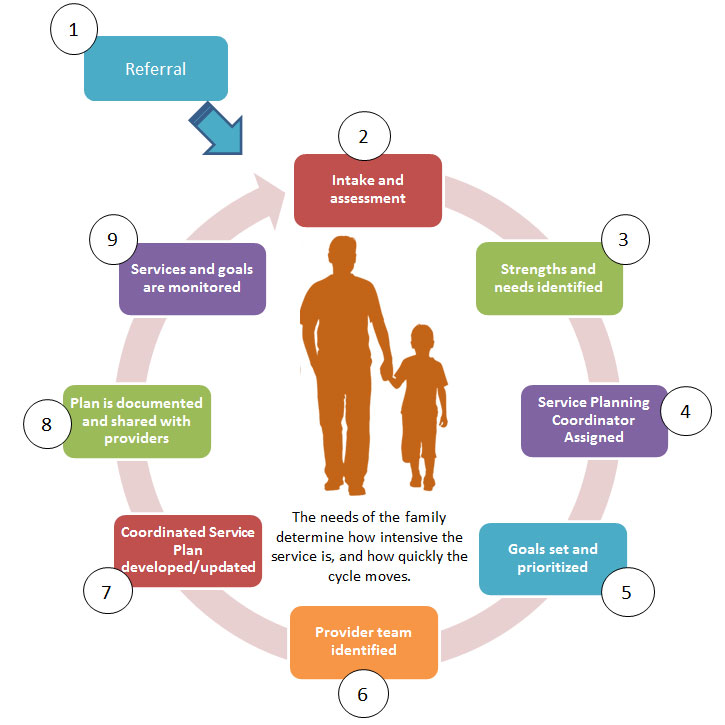
Diagram showing the nine steps to the Coordinated Service Planning Cycle. The steps circle around a silhouette of a parent holding a child’s hand. Under the parent and child, a caption says that the needs of the family determine how intensive the service is and how quickly the cycle moves.
- 1. Referral
- This first step is outside of the circle as it identifies how families enter the Coordinated Service Planning Cycle. There is an arrow pointing towards Step 2: Intake and assessment in the cycle.
- Intake and assessment
- Strengths and needs identified
- Service Planning Coordinator assigned
- Goals set and prioritized
- Provider team identified
- Coordinated Service Plan developed/updated
- Plan is documented and shared with providers
- Services and goals are monitored
- This step is followed by an arrow that points towards Step 2: Intake and assessment showing that the circle continues.
A family’s file may be made inactive at any time during the cycle when the family and service provider decide that Coordinated Service Planning is no longer needed by the family.
A family can re-engage with Coordinated Service Planning if new needs develop or circumstances change.
The following describes, in further detail, the Coordinated Service Planning cycle, the key steps in the delivery of Coordinated Service Planning. This section illustrates the common service experience a family should be able to expect from Coordinated Service Planning across the province.
1. Referrals to Coordinated Service Planning
Referrals to Coordinated Service Planning can be made at any point a child/youth’s needs are recognized to be multiple and/or complex. This could either be:
- early on, when developmental concerns are first identified, or
- when the family’s situation changes, when new needs are identified, or when new services are added.
When any special needs service provider (and/or broader sector partner such as healthy child development, healthcare and child care providers as well as educators) recognizes that a family may need Coordinated Service Planning, they should explain what Coordinated Service Planning is and why it may be beneficial to the family. If the family is interested, with consent, their information will be shared with the Coordinating Agency for intake through a warm referral. Families can also self-refer to Coordinated Service Planning.
Referrals will, with consent, include information about the child and family, in order to ensure that the need for the family to repeat their story is minimized. At a minimum, this should include:
- basic information about the family (names, contact information)
- information about their strengths, needs and circumstances
- child/youth’s strengths, needs and services
Referrals to Coordinated Service Planning should be made in parallel to referrals to other services, particularly if there is a wait for Coordinated Service Planning. Being referred to Coordinated Service Planning should not prevent a family from accessing other appropriate services. Coordinated Service Planning is not a required point of access or a gatekeeper and Service Planning Coordinators are not responsible for determining eligibility for other programs
2. Intake and Assessment
When a family is referred to Coordinated Service Planning, they will be assessed to determine whether they should receive Coordinated Service Planning and at what intensity.
The Coordinating Agency will establish an intake procedure that allows a Service Planning Coordinator and/or other trained individual to work with the family to assess the family’s needs and identify whether they should receive Coordinated Service Planning (see Part 3 for more detail on characteristics of the child/youth and family to consider when making this determination).
Service Intensity
Coordinated Service Planning will be delivered at varying levels of intensity. When making a determination about whether a family should receive Coordinated Service Planning, the intensity at which the service will be provided should also be assessed (informed by family needs, strengths, and capacity):
- Brief supports – e.g. a Coordinated Service Plan developed and brief, time-limited supports from a Service Planning Coordinator
- Intermittent support – e.g. more intensive level of support during transitions and less intensity at other times
- Continuous supports
Decisions regarding how frequently a Service Planning Coordinator is engaged and how frequently the Coordinated Service Plan is reviewed and updated will be made jointly by the child/youth and family with the Service Planning Coordinator.
Family capacity may also change over time. Some families will develop the capacity for and interest in coordinating their own services, while others may access Coordinated Service Planning for the first time as a result of a transition or a change in the family’s circumstances.
If the family must be placed on a waitlist for Coordinated Service Planning
Because Coordinated Service Planning is not a mandatory service, Coordinating Agencies may manage waitlists for Coordinated Service Planning if demand exceeds capacity. When multiple agencies are delivering Coordinated Service Planning in the service delivery area, there will be a single waitlist for Coordinated Service Planning (understanding that in large service delivery areas there may be regional sub-lists).
Families will be placed on a waitlist based on the date of first contact with the Coordinating Agency (i.e. during the intake process). When families with inactive plans need to re-engage with Coordinated Service Planning, they may be prioritized for access to a Service Planning Coordinator over families on the waitlist. Coordinating Agencies may develop further prioritization criteria or exceptions, for example prioritizing families who have plans from another service delivery area and have recently moved, families with needs requiring immediate response, or families in crisis.
3. Family strengths and needs are identified
The child/youth and his or her family are at the centre of Coordinated Service Planning. When a plan is initiated, the Service Planning Coordinator will gather key information about the child/youth and family through the following:
- discussion with the child/youth and family
- information shared by other service providers
- conducting a strengths and needs assessment
A strengths-based approach will be used to inform the development of the Coordinated Service Plan, including areas where children/youth and their families have strengths and areas where they could be supported. These can be functional strengths such as behaviour and problem-solving skills; or family, cultural and community strengths, for example the involvement of members of the extended family. A family’s ties to a cultural community such as a First Nations, Métis, Inuit and urban Indigenous community should be identified as part of the strengths assessment to inform the Coordinated Service Planning process.
Family strengths and needs should be monitored and updated at regular intervals. As the needs and strengths of a family change over time, the intensity at which Coordinated Service Planning is delivered may be adjusted.
4. Assigning a Service Planning Coordinator
A relationship with a Service Planning Coordinator may be developed as part of the process of identifying and assessing needs and strengths. By the time a family is ready to set goals, a Service Planning Coordinator must be formally assigned/identified. Service Planning Coordinator assignments should take into account:
- family preferences
- existing relationships
- their needs assessment (because specific experience or expertise may be required)
- other factors (e.g. linguistic or cultural needs)
Families should be made aware who their Service Planning Coordinator is, what their role is, and that they are the key contact for questions about the plan.
5. Family and/or child/youth goals are set and prioritized
The family’s circumstances, preferences, knowledge of their child/youth and goals will be the foundation of the planning. The child/youth’s voice, preference and goals will also be central to Coordinated Service Planning, particularly as they mature and begin to prepare for adulthood.
Goal setting will be based on what the family and/or child/youth sees as the most important. Goals can be related to specific activities, therapies, or other domains of development (e.g. feeding oneself, attending a birthday party). Goals can also be prioritized based on what is most urgent for the family.
Initial goal setting can be done by the child/youth and his/her family with the Service Planning Coordinator or with the full provider team. Families and/or the child/youth (as appropriate) have the final decision over which goals are included in the plan.
6. Provider team is identified
A team meeting may be needed to develop the plan. Family members (parents/guardians), and child/youth as appropriate, are critical partners in Coordinated Service Planning and should be identified as equal members of the team. With family and/or child/youth consent, the team may include providers from outside the children’s services sectors, e.g. from school, healthcare, child welfare. Examples of service providers that may be included are:
- speech and language therapists
- behavioural therapists
- occupational therapists
- special education teachers or other educators
- social workers
- healthcare care coordinator
Not all professionals involved in the child’s services need to be at meetings, depending on the circumstances, the child/youth’s needs, and the preference of the family. Families and/or the child/youth will determine which service providers should be invited to the meeting.
The team meeting should be held in a place that will be comfortable and accessible for the family. Supports to aid family involvement (e.g. a translator, support person, conferencing services) should be made available. Families are the critical player on the team, because they can provide information on their child/youth’s interests, strengths, needs, and history that will form the foundation of the plan.
7. Coordinated Service Plan is developed
The Coordinated Service Plan is a written document for a child/youth with multiple and/or complex special needs and his/her family, as well as all service providers involved in his or her care. At minimum, the Coordinated Service Plan will contain the following:
- General information about the child/youth and family
- Information about the child/youth and family’s strengths, needs and interests
- Child/youth and family vision/priorities (e.g. what is most important to the child/youth and family; what are their longer-term aspirations?)
- List of provider team members/agencies involved in providing service to the child/youth and their roles
- Goals, how each goal will be achieved and who is responsible for what
Families and/or the child/youth should determine which services are included in the plan with the support of the Service Planning Coordinator. The Coordinated Service Plan should aim to encompass every type of service that will be required by, or would be beneficial for the child/youth
Families can expect their Coordinated Service Plan to be a living document that grows and develops with their child/youth. The plan belongs to the family, and the Service Planning Coordinator monitors it on their behalf and works with them to update it. The needs and goals of children/youth and families will change over time, and so will their Coordinated Service Plan.
The goals and the vision of the Coordinated Service Plan should inform, and be informed by, all planning for services, supports and special education, including the Individual Education Plan
Services are planned to meet goals
Families and/or the child/youth should clearly understand how services are being planned to meet the agreed-upon goals. Providers are encouraged to draw connections between services and articulate these to the family and/or child/youth. Service providers determine what services they will provide based on the policy/program requirements and their clinical judgment.
Service Planning Coordinators will work with the child/youth, families and providers to make sure families have the information they need to make informed decisions about services. It is the responsibility of the Service Planning Coordinator to understand, monitor, and document how services will support the achievement of the prioritized goals.
Coordinated Service Planning will be focused on the needs of the child/youth with complex and/or multiple special needs; however, Service Planning Coordinators should be aware of other needs the family has and should be able to make referrals to relevant services. The Service Planning Coordinator has the discretion to assist the family to help the child or youth achieve his or her outcomes, but is not required to coordinate services for the family that are outside the scope of Coordinated Service Planning.
8. Plan is shared with family and providers
Once the Coordinated Service Plan has been documented, the plan will be shared with child/youth and their family. The final decision about who should see the plan, or specific parts of the plan, rests with the family and/or child/youth.
With the consent of the family, it is the responsibility of the Service Planning Coordinator to make sure that the Coordinated Service Plan is shared with the relevant service providers. Service Planning Coordinators are responsible for communicating, with consent, about the child/youth’s needs, strengths, family/youth’s goals and priorities to service providers and educators.
9. Services and goals are monitored
In addition to regular communication with families, service providers should inform families that they can contact their Service Planning Coordinator when they:
- have a question about the plan
- think the plan should be adjusted
- want to adjust goals
- require additional supports
- need a new service
Service Planning Coordinators will make referrals/connections as new needs and potential supports are identified and/or call meetings with service providers when the family indicates that their goals have changed or that the plan needs to be adjusted. Where possible, the Service Planning Coordinator should connect with the provider on behalf of the family and facilitate a warm referral.
At a minimum, the Coordinated Service Plan will be reviewed with the child/youth and family every six months. Goals will be revisited and confirmed or revised each time the plan is reviewed.
Some families may require more frequent updates at varying times. Plans should be updated more frequently around transitions in the child/youth’s circumstances or services, for instance, upon transition into school, high school or adulthood (see Part 5: Transitions).
Depending on the needs of the child/youth and family, at times, Coordinated Service Planning may be more intensive and the cycle may move more quickly.
Inactivity and/or Discharge
Families may have periods where they need little to no Coordinated Service Planning, or come to a point where the family no longer wishes to access Coordinated Service Planning. In these situations, Coordinating Agencies may wish to categorize these plans as inactive, or consider discharge.
Inactive Plans
Plans may be categorized as inactive if there is no immediate need for service but the family would like the option to access Coordinated Service Planning at a future time. Plans will be categorized as inactive when there is no need for re-assessment, active planning or regular review of the Coordinated Service Plan.
Service Planning Coordinators will advise families that they may re-engage with Coordinated Service Planning again if their needs change (until the age of 21, if the youth remains in school). With consent, the Coordinating Agency will retain inactive files so that families may re-engage with Coordinated Service Planning, as needed, without having to repeat the intake process.
- The Coordinating Agency may take a coaching approach with families and other providers and a gradual approach to stepping down service prior to categorizing a plan as inactive.
- Agencies may wish to reach out to these families at anticipated transition points (e.g. entry to school, entry to adolescence or high school) to inform them they may re-enter Coordinated Service Planning to support them through the transition.
- I will not report families with inactive plans to the ministry as being in receipt of service.
Discharging
Youth are eligible for Coordinated Service Planning until the age of 18, or until the age of 21 if they remain in school. In addition to age, an agency should consider discharge when:
- Goals are met and the family and team is satisfied that Coordinated Service Planning is no longer required;
- The family leaves the catchment area. The agency will provide a warm referral and the current plan to the local Coordinating Agency in the new catchment area (with the consent of the family). The family should not be reassessed;
- The family cannot be reached after four documented attempts over two quarters through the best method of contact indicated by the family (families are expected to keep current contact information on file with the agency while they are receiving service); or
- The family requests discharge.
Footnotes
- footnote[4] Back to paragraph Children/youth with multiple and/or complex special needs are expected to have a Coordinated Service Plan and the support of a Service Planning Coordinator prior to accessing service resolution processes. See Part 7: Service Resolution.
- footnote[5] Back to paragraph May include therapy/rehabilitation, health services (including nursing), special education, respite, etc.
- footnote[6] Back to paragraph The Coordinated Service Plan should complement, not replace, the child/youth’s Individual Education Plan (IEP), and may be used as one source of information to help inform education program planning, including special education programming and/or services that a child/youth may need.